Eina! Study shows hospitals are botching pain management
Most patients do not receive important treatment during and after surgery
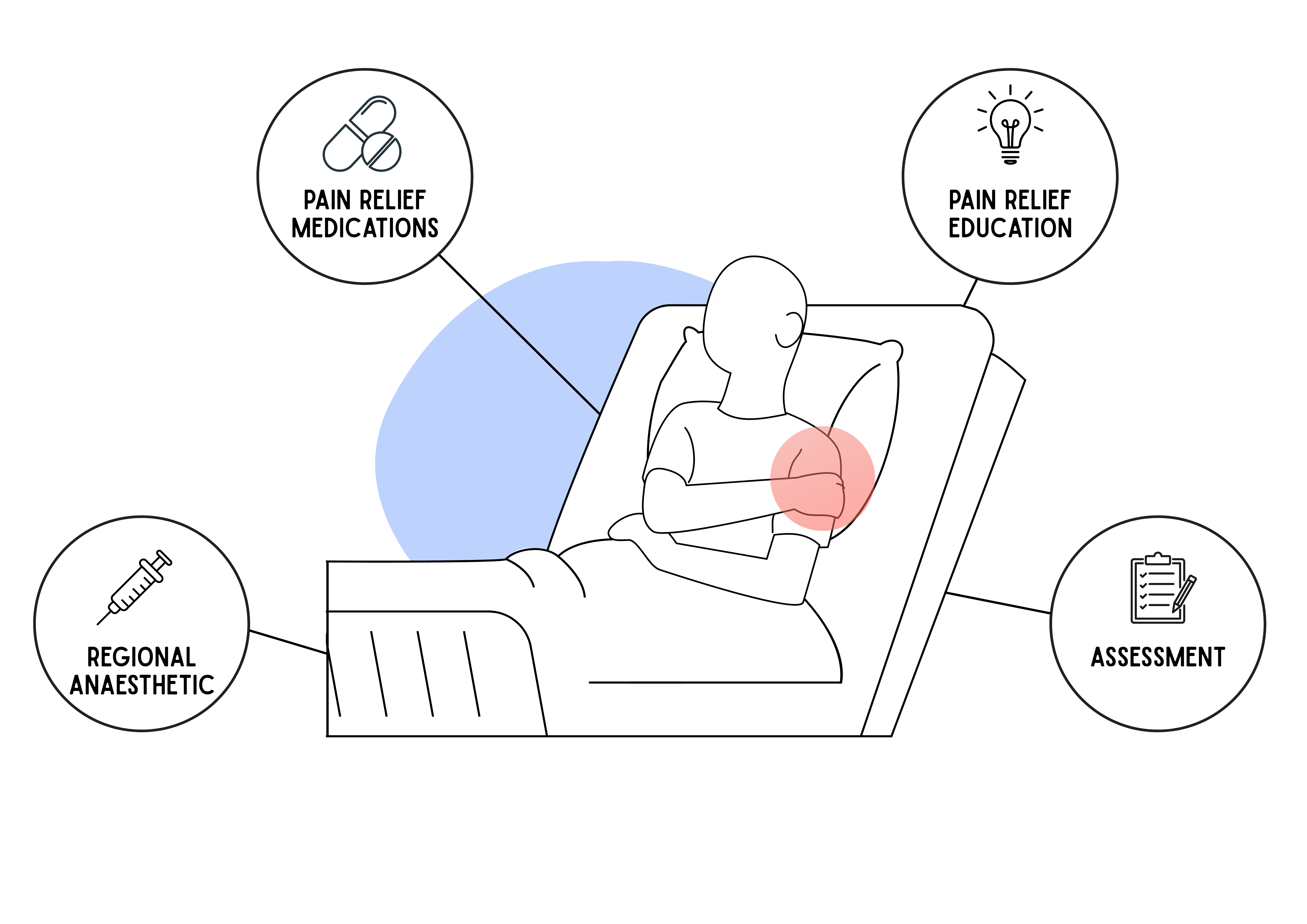
Graphic depicting the four elements of pain management. Illustration: Lotte Manicom
A paper published on Friday by Lancet Africa provides disturbing insight into the way acute pain is managed in South African hospitals during and after surgery.
Pain is divided into two broad types: acute and chronic. Acute pain is short and intense, the type you would experience after surgery. Chronic pain lasts more than three to six months, sometimes longer, after an initial injury has healed. This study looked at acute pain.
The researchers considered data from over 3,500 patients across five surgical disciplines at ten hospitals. They wanted to know how widely four important aspects of acute pain management were implemented. These are:
- Patients are educated on how to manage their pain.
- Patients receive pain relief for the area around their wound, in addition to the main operation.
- Patients receive pain relief medications during and after the operation.
- Pain is assessed in patients after their operations.
The researchers first used patient records taken from September 2021 to April 2022 to estimate how widely the above bundle of care was implemented. Only 9% of patients received all four interventions.
“It’s the first time that we’ve got big data showing that acute pain is a real problem in this population, and we’re doing a pretty shitty job of dealing with it,” says lead author Professor Romy Parker, Director of the Pain Management Unit at the University of Cape Town.
“The good news is that it doesn’t take rocket science or millions of rands to make a difference. It just takes paying attention.”
Researchers at the hospitals that the data was obtained from met in June 2022. Everyone agreed to implement the four-element bundle. Patients would be given education and receive at least a combination of paracetamol (commonly branded as Panado) and non-steroidal anti-inflammatories (such as ibuprofen).
“We found that with these relatively simple things you can make quite a big difference to people’s pain management. Patients’ pain reduced from being moderate, the kind of pain that interferes with your movement, mood and cognition, to mild, the kind of pain which is a bit annoying but doesn’t stop you from doing all the things you need to and want to do,” says Parker.
The researchers then evaluated data taken from January to April 2023.
Care improved a bit: 39% of patients received all four interventions.
Parker says the gold standard in quality improvement studies is to get 80% adherence to the changes.
“We fell way short of that, mostly because getting people to change their behaviour is hard! We think it is promising, though, because the improvement was achieved in just three months, with no resources at all. No extra funding, no dedicated training time, no system changes, just teamwork. Imagine what we could do with a structured and supported approach – management support, funding for training and implementation and staff dedicated to supporting the behaviour change,” she says.
Managing acute pain reduces burden on health system
“Acute pain on its own is a fairly straightforward problem, which typically fades as the injury heals,” explains Associate Professor Sean Chetty, a senior author on the paper and head of the Department of Anaesthesiology and Critical Care at the University of Stellenbosch’s Faculty of Medicine and Health Sciences.
“The problem comes when acute pain is not properly managed. When this happens, acute pain can transition into chronic pain, which is a much more invidious thing. Chronic pain destroys lives, and even impacts the state in the form of increased disability grants and so on. If we can approve the management of acute peri-operative pain, we can potentially lessen our burden of chronic pain.”
Main results of the study
This table shows what percentage of patients received between 0 (none) and four (all) of the interventions in the first analysis (before the meeting of June 2022) and the second analysis (after the June 2022 meeting). Percentages are rounded, so may not add precisely to 100.
|
Interventions received |
% of patients receiving intervention in first analysis |
% of patients receiving intervention in second analysis (after June 2022 meeting) |
|
0 |
1 |
1 |
|
1 |
14 |
4 |
|
2 |
38 |
17 |
|
3 |
38 |
40 |
|
4 |
9 |
39 |
Support independent journalism
Donate using Payfast
![]()
Don't miss out on the latest news
We respect your privacy, and promise we won't spam you.
© 2026 GroundUp. This article is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
You may republish this article, so long as you credit the authors and GroundUp, and do not change the text. Please include a link back to the original article.
We put an invisible pixel in the article so that we can count traffic to republishers. All analytics tools are solely on our servers. We do not give our logs to any third party. Logs are deleted after two weeks. We do not use any IP address identifying information except to count regional traffic. We are solely interested in counting hits, not tracking users. If you republish, please do not delete the invisible pixel.