In pain? You might have to suck it up
“The difference between public and private [health sectors] is like night and day when it comes to managing acute pain”
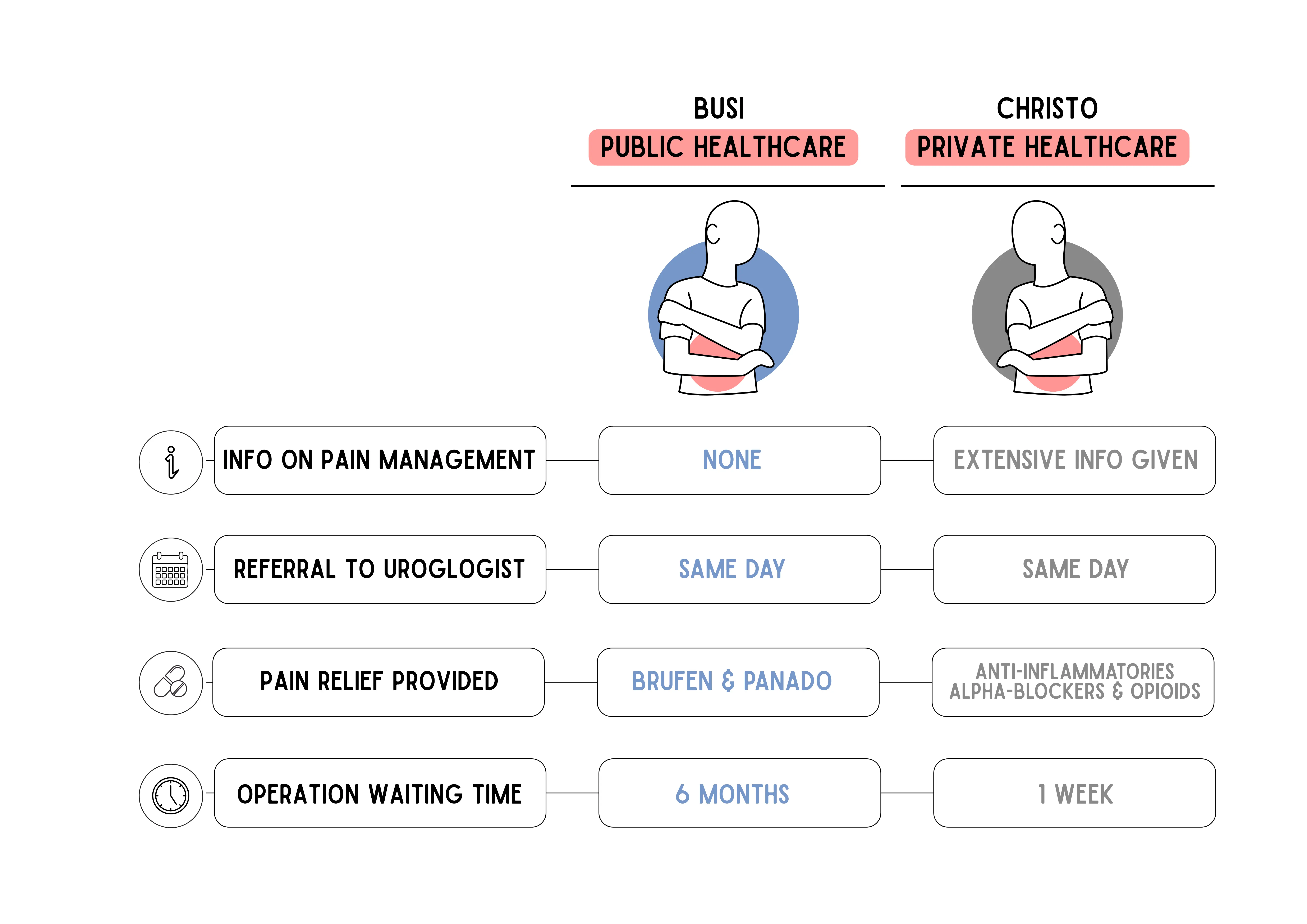
Busi and Christo both had acute pain from kidney stones. But Busi used the public health system and Christo went private. How they were treated was very different. Illustration: Lotte Manicom
- Two patients had kidney stones. One used the public health system. One used the private system. Their outcomes were very different.
- Management of acute pain in the South African public health system is poor. A study published on 13 March in Lancet Africa confirms this.
- One of the researchers on that study says: “The good news is that it doesn’t take rocket science or millions of rands to make a difference.”
Busi has been in agony. It started in October 2025, a severe pain in her side, shooting down between her legs.
“More than childbirth” is how she describes it.
Busi asked a family member to take her straight to the Emergency Room at Livingstone Hospital in Gqeberha. She was assessed and referred to the hospital’s urology department, which diagnosed a two-centimetre stone in the urine drainage system of one of her kidneys. A stent was put in to alleviate pain, and Busi was booked for surgery in April 2026.
The unbearable pain continued; a problem with the stent it seemed. The anti-inflammatories and paracetamol she was given to manage her pain helped very little. In desperation, she booked an appointment with a doctor in private practice, who gave her morphine and tried to get her operation date brought forward but without success.
“He even sent me to East London, which is not the referral network for this part of the world, but they were booked until next year [2027]. Until then, my life is on pause, I cannot go anywhere. I cannot be a mother and wife,” says Busi.
In February, Gqeberha resident Christo was driven to hospital with a similar problem.
“A stent was put in the next day, and I was booked for surgery the next week. In the interim I was given excellent painkillers,” says Christo.
He has recovered from his surgery and says he is pain free.
The difference between the two outcomes was private medical insurance. Christo, who is insured, reported to a private hospital in which several urologists work, all with manageable case volumes and access to a range of pain management medicines that are not available in the state health system.
(Busi and Christo are not their actual names.)
“The difference between public and private [health sectors] is like night and day when it comes to managing acute pain,” says Dr Ben Gaunt, formerly the CEO of Zithulele Hospital near Mquanduli and now a general practitioner in private practice in Port Alfred.
“In state healthcare, whether your pain is acute or chronic, you typically get Panado [paracetamol], Brufen [ibuprofen], and if you’re lucky something a little bit stronger. There are strong and weak opioids on the Essential Medicines List but a lot of district hospitals can’t access them. And even if they can, staff are often ignorant on how to use them,” he says.
When he was running Zithulele, Gaunt co-wrote a paper showing that health professionals in rural state hospitals are often fearful of using morphine.
“Even patients who were very near the end of life were being under-dosed, so it raises a question of the confidence of practitioners in managing pain. And for those who are competent, can they get access to the right painkillers for the type of pain they are trying to treat? The answer is typically, no, they can’t. The reality is that pain management in most of South Africa is terrible, and we rely on the fact that our patients are unbelievably tough,” says Gaunt.
Health professionals typically differentiate between two broad categories of pain: acute pain, which is short and intense, the type of pain one would experience after surgery, and chronic pain, lasting more than three to six months, and sometimes persisting long after an initial injury has healed.
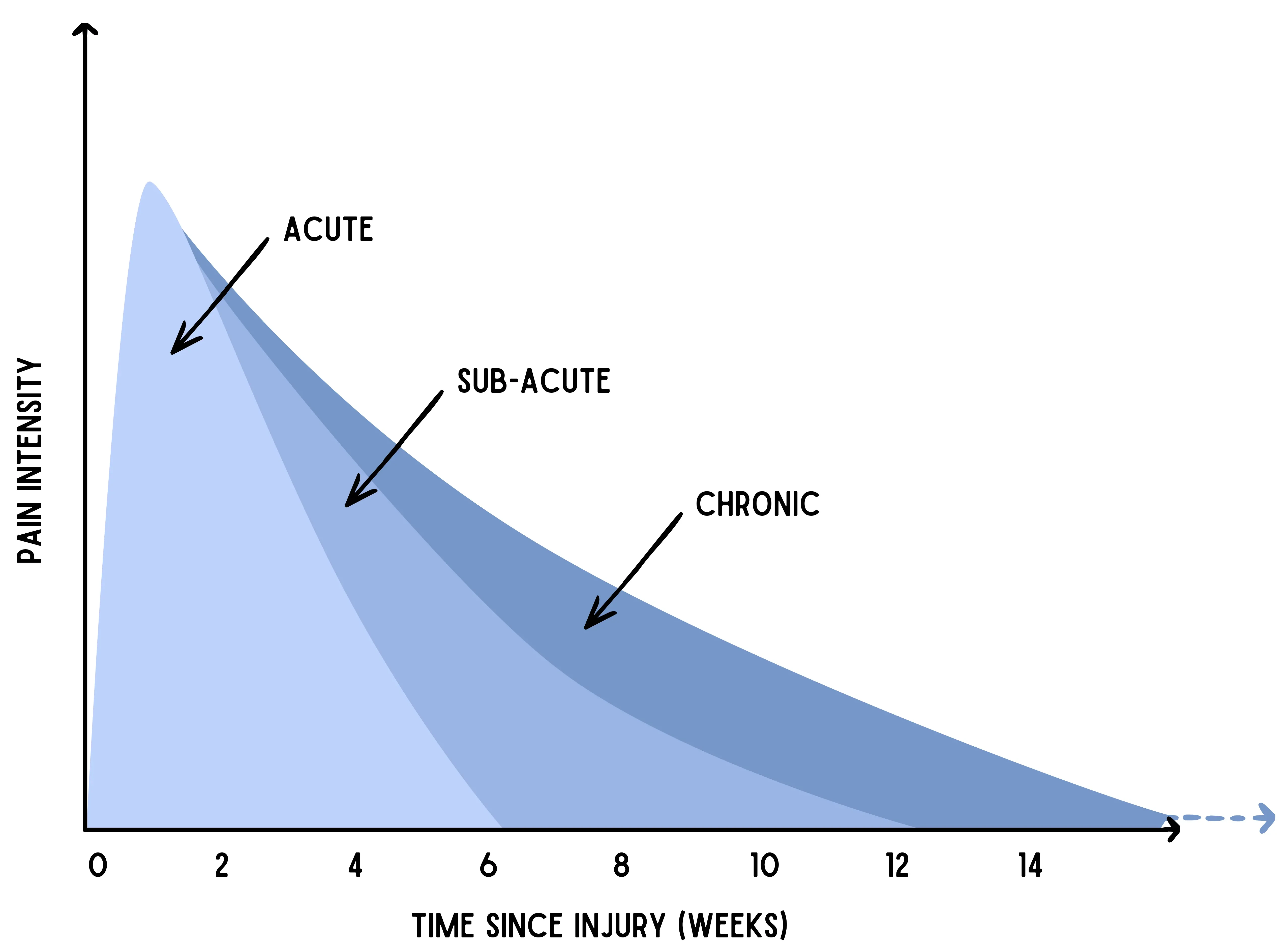
Graph adapted from J Park-Ross and R Parker’s book Understanding Pain: Unravelling the Physiology, Assessment, and Management of Pain through South African Stories (2024)
“Acute pain on its own is a fairly straightforward problem, which typically fades as the injury heals,” says Dr Sean Chetty, head of anaesthesiology and critical care at Stellenbosch University’s medical faculty. “However, when acute pain is not properly managed it can transition into chronic pain, which is a more invidious thing.”
“Chronic pain destroys lives, and even impacts the state in the form of repeat clinic visits, increased disability grants and so on. If we can improve the management of acute pain, we can potentially lessen our burden of chronic pain,” says Chetty.
In North West Province, department heads in several district hospitals told GroundUp that they have no access to basic acute pain management tools such as IV bags combining paracetamol and opioids, as well as paracetamol in combination with non-steroidal anti-inflammatories (such as ibuprofen).
“These things are on the essential medicines list but the department doesn’t like to buy them, primarily for reasons of cost, so most patients – even paediatric patients - are now put on opiates such as Tramadol as alternatives, which is problematic especially since there is no evidence that Tramadol is safe in children,” said one clinician based at Tshepong Hospital in Klerksdorp, citing departmental communications policy as a reason for remaining anonymous.
A study on surgery pain management in ten South African hospitals, published on 13 March by Lancet Africa, provides further insight into the poor management of acute pain. The researchers used patient records taken from September 2021 to April 2022 in ten hospitals (eight public and two private) to estimate how widely were certain basic pain relief measures being implemented. They found that only one in two patients received information on pain management, while one in three received non-opioid painkillers during and after surgery.
“It’s the first time that we’ve got big data showing that acute pain is a real problem in this population, and we’re doing a pretty shitty job of dealing with it,” says lead author Professor Romy Parker, director of the pain management unit at the University of Cape Town.
She says, “The good news is that it doesn’t take rocket science or millions of rands to make a difference, it just takes paying attention. We found that by doing simple things like making sure patients receive a combination of Panado and non-steroidal anti-inflammatories, and giving patients education about the things they can do themselves to manage their pain, you can make quite a big difference to people’s pain management.
“Patients’ pain reduced from being moderate, the kind of pain that interferes with your movement, mood and cognition, to mild, the kind of pain which is a bit annoying but doesn’t stop you from doing all the things you need to and want to do.”
Support independent journalism
Donate using Payfast
![]()
Don't miss out on the latest news
We respect your privacy, and promise we won't spam you.
Next: SA Human Rights Commission must compel government to end hunger, activists demand
Previous: Shosholoza Meyl faces uncertain future
© 2026 GroundUp. This article is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
You may republish this article, so long as you credit the authors and GroundUp, and do not change the text. Please include a link back to the original article.
We put an invisible pixel in the article so that we can count traffic to republishers. All analytics tools are solely on our servers. We do not give our logs to any third party. Logs are deleted after two weeks. We do not use any IP address identifying information except to count regional traffic. We are solely interested in counting hits, not tracking users. If you republish, please do not delete the invisible pixel.